Fertility Selection in the Rh-factor system of humans
The Rh
blood-type is due to the presence or absence
of a RBC-surface antigen coded by an
allele at the RHD locus on Chromosome
1. When the R allele
is present in either homozygous or heterozygous phase (RR or
Rr, respectively), the antigen produces the Rh+ phenotype.
In the absence of the antigen, rr homozygotes show
the Rh- phenotype. R is
thus dominant to r. Rh
phenotypes are typically reported together with the ABO blood-type:
the most common blood-type in persons of European ancestry is
O+.
One type of Hemolytic Disease of Newborns (HDN) occurs when the father is RR or Rr (Rh+), the mother is rr (Rh-), and she gives birth to a child with an RR or Rr blood type. The fetal R antigen sensitizes the mother to produce anti-Rh+ antibodies. Typically, the first Rh+ pregnancy only sensitizes the rr mother, and the fetus is not at risk. However, subsequent pregnancies and fetuses are at severe risk, because the anti-Rh+ antibody titre has been raised by the first fetus, and the antibodies attack fetal blood cells early in pregnancy. The result is HDN, which causes spontaneous abortion, stillbirth, or a severely anemic newborn. If the at-risk parental Rh blood types are known before pregnancy, prophylactic treatment of the mother during the first pregnancy with IgG immune-suppressors such as Rhogam prevents development of the antibody, and the pregnancy can proceed to term. Treatment must be repeated at each subsequent pregnancy, and is ineffective if not applied at the time of the first, sensitizing pregnancy.
Besides the immediate medical concerns for individuals, the Rh system has consequences for population and evolutionary genetics.
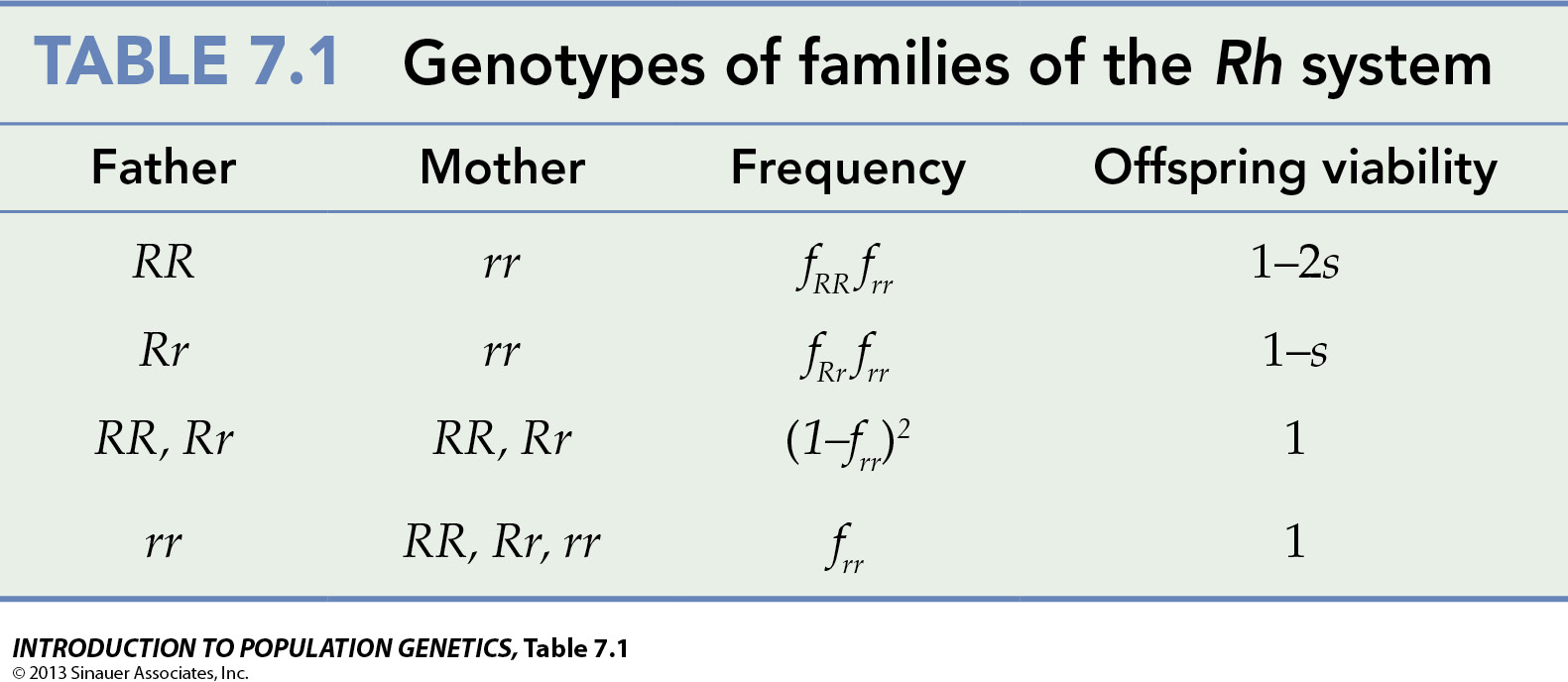
(I) For any individual pregnancy, risk probabilities are calculated from Mendelian first principles, as shown in the table: if the mother is rr, 100%, 50%, and 0% of fetuses with RR, Rr, and rr fathers, respectively, are at risk. Where the mother is RR or Rr, none of the fetuses are at risk, no matter the genotype of the father. Thus the genetic counseling question arises always & only when the mother is Rh- [See Note on Genetic Counseling below]. Most provinces and states require an Rh test for a marriage license.
(II) In terms of population genetics, if we want to calculate the fraction of the population at risk, we require knowledge of the frequency f of each of the three genotypes, fRR, fRr, and frr. The selection scheme is additive selection: half of the fetuses of Rr x rr mothers are at risk, which is equivalent to a selection coefficient of (1-s). All of the fetuses of RR x rr mothers are at risk, and the fitness of such marriages is (1-2s).
The novel mode of selection here is that fetuses with identical Rr genotypes have different viability, according to the maternal environment. Mothers with identical rr genotypes have different fertility, according to the father's genotype.
(III) In terms of evolutionary genetics, different population have different frequencies of the two alleles, and alternative outcomes are expected if either R or r is rare.
(1) If R is relatively rare [say, f(R) = 0.1], relatively few men are Rh+, and most of these are Rr: f(Rr) = (2)(0.1)(0.9) = 0.18 versus f(RR) = 0.12 = 0.01. A large majority of women are Rh- [f(rr) = 0.92 = 0.81]. The proportion of marriages between Rh+ men and Rh- women is then (0.18)(0.81) = 0.146 of the total, which marriages will be at a selective disadvantage (1 - s) to marriages between Rh- men and Rh- women [proportion (0.81)(0.81) = 0.656 with no selective disadvantage (s = 0). Selection acts effectively only on Rh+ men, and the expectation is that f(R), already rare, will decrease further.
(2) If r is relatively rare [say, f(r) = 0.1], almost all women are Rh+ [f(RR) = 0.92 = 0.81 or f(Rr) = (2)(0.9(0.1) = 0.18, total 0.99] and never subject to selection (s = 0). Expected blood type frequencies among men are the same. These women will be at a selective advantage relative to the rare Rh- women [f(rr) = 0.12 = 0.01], most of whom will marry Rh+ men [(0.01)(0.81 + 0.18) ~ 0.01], and therefore be at a selective disadvantage (typically 1 - 2s). As in III.1 above, RR or Rr men who marry rr women will be at a selective disadvantage, as they are expected to have fewer viable offspring. The expectation is that f(r) will decrease further. As we have seen however, this selection is inefficient against a rare recessive rr genotype.
Thus, when either R or r is rare, selection ought to decrease its frequency further: the residual polymorphism is unstable and selection is disruptive. The fact that many human populations are polymorphic for the Rh-factor blood-type suggests that something else is going on. One suggestion is that alternative Rh types were (pre)-historically favored in different, separated populations, so that the polymorphism now observed within populations was originally maintained among polytypic populations, and that human history has only recently allowed these populations to interbreed.
[Note on Genetics Counseling: Explanations of the Mendelian genetics of single-locus medico-genetic conditions is the least of it. Counselors must address the tendency of one partner or the other to assign or assume blame for allelic combinations that pre-dispose towards the condition. This is strongly influenced by societal norms. In case (I) above, there is sometimes a tendency to 'blame the Mother', because HDN is limited to the fetuses of the rr maternal genotype. Phrased alternatively, because HDN arises only by the combination of a paternal R with an r from an rr mother, an Rr father has an affected child by chance, and this might be seen as shifting the onus to the Father. Secondary questions are raised in the marriage of an RR father x rr mother, where all pregnancies will be affected and prophylactic treatment is mandatory, or marriages of an Rr father x rr mother where pre-natal testing is (arguably) necessary, followed by prophylactic treatment as required. Tertiary questions arise in the case of unplanned pregnancy, spontaneous or planned abortion, especially if the genotype of the father is unknown, in which case sensitization may occur with prior knowledge].
One type of Hemolytic Disease of Newborns (HDN) occurs when the father is RR or Rr (Rh+), the mother is rr (Rh-), and she gives birth to a child with an RR or Rr blood type. The fetal R antigen sensitizes the mother to produce anti-Rh+ antibodies. Typically, the first Rh+ pregnancy only sensitizes the rr mother, and the fetus is not at risk. However, subsequent pregnancies and fetuses are at severe risk, because the anti-Rh+ antibody titre has been raised by the first fetus, and the antibodies attack fetal blood cells early in pregnancy. The result is HDN, which causes spontaneous abortion, stillbirth, or a severely anemic newborn. If the at-risk parental Rh blood types are known before pregnancy, prophylactic treatment of the mother during the first pregnancy with IgG immune-suppressors such as Rhogam prevents development of the antibody, and the pregnancy can proceed to term. Treatment must be repeated at each subsequent pregnancy, and is ineffective if not applied at the time of the first, sensitizing pregnancy.
Besides the immediate medical concerns for individuals, the Rh system has consequences for population and evolutionary genetics.
(I) For any individual pregnancy, risk probabilities are calculated from Mendelian first principles, as shown in the table: if the mother is rr, 100%, 50%, and 0% of fetuses with RR, Rr, and rr fathers, respectively, are at risk. Where the mother is RR or Rr, none of the fetuses are at risk, no matter the genotype of the father. Thus the genetic counseling question arises always & only when the mother is Rh- [See Note on Genetic Counseling below]. Most provinces and states require an Rh test for a marriage license.
(II) In terms of population genetics, if we want to calculate the fraction of the population at risk, we require knowledge of the frequency f of each of the three genotypes, fRR, fRr, and frr. The selection scheme is additive selection: half of the fetuses of Rr x rr mothers are at risk, which is equivalent to a selection coefficient of (1-s). All of the fetuses of RR x rr mothers are at risk, and the fitness of such marriages is (1-2s).
The novel mode of selection here is that fetuses with identical Rr genotypes have different viability, according to the maternal environment. Mothers with identical rr genotypes have different fertility, according to the father's genotype.
(III) In terms of evolutionary genetics, different population have different frequencies of the two alleles, and alternative outcomes are expected if either R or r is rare.
(1) If R is relatively rare [say, f(R) = 0.1], relatively few men are Rh+, and most of these are Rr: f(Rr) = (2)(0.1)(0.9) = 0.18 versus f(RR) = 0.12 = 0.01. A large majority of women are Rh- [f(rr) = 0.92 = 0.81]. The proportion of marriages between Rh+ men and Rh- women is then (0.18)(0.81) = 0.146 of the total, which marriages will be at a selective disadvantage (1 - s) to marriages between Rh- men and Rh- women [proportion (0.81)(0.81) = 0.656 with no selective disadvantage (s = 0). Selection acts effectively only on Rh+ men, and the expectation is that f(R), already rare, will decrease further.
(2) If r is relatively rare [say, f(r) = 0.1], almost all women are Rh+ [f(RR) = 0.92 = 0.81 or f(Rr) = (2)(0.9(0.1) = 0.18, total 0.99] and never subject to selection (s = 0). Expected blood type frequencies among men are the same. These women will be at a selective advantage relative to the rare Rh- women [f(rr) = 0.12 = 0.01], most of whom will marry Rh+ men [(0.01)(0.81 + 0.18) ~ 0.01], and therefore be at a selective disadvantage (typically 1 - 2s). As in III.1 above, RR or Rr men who marry rr women will be at a selective disadvantage, as they are expected to have fewer viable offspring. The expectation is that f(r) will decrease further. As we have seen however, this selection is inefficient against a rare recessive rr genotype.
Thus, when either R or r is rare, selection ought to decrease its frequency further: the residual polymorphism is unstable and selection is disruptive. The fact that many human populations are polymorphic for the Rh-factor blood-type suggests that something else is going on. One suggestion is that alternative Rh types were (pre)-historically favored in different, separated populations, so that the polymorphism now observed within populations was originally maintained among polytypic populations, and that human history has only recently allowed these populations to interbreed.
[Note on Genetics Counseling: Explanations of the Mendelian genetics of single-locus medico-genetic conditions is the least of it. Counselors must address the tendency of one partner or the other to assign or assume blame for allelic combinations that pre-dispose towards the condition. This is strongly influenced by societal norms. In case (I) above, there is sometimes a tendency to 'blame the Mother', because HDN is limited to the fetuses of the rr maternal genotype. Phrased alternatively, because HDN arises only by the combination of a paternal R with an r from an rr mother, an Rr father has an affected child by chance, and this might be seen as shifting the onus to the Father. Secondary questions are raised in the marriage of an RR father x rr mother, where all pregnancies will be affected and prophylactic treatment is mandatory, or marriages of an Rr father x rr mother where pre-natal testing is (arguably) necessary, followed by prophylactic treatment as required. Tertiary questions arise in the case of unplanned pregnancy, spontaneous or planned abortion, especially if the genotype of the father is unknown, in which case sensitization may occur with prior knowledge].
Figure © 2013 by Sinauer; Text material © 2024 by Steven M. Carr