Down Syndrome (Trisomy-21) (2n = 47, +21)
Down Syndrome
(Trisomy-21)
occurs as a results of non-disjunction of
chromosomes during meiosis, such that the gamete contributed
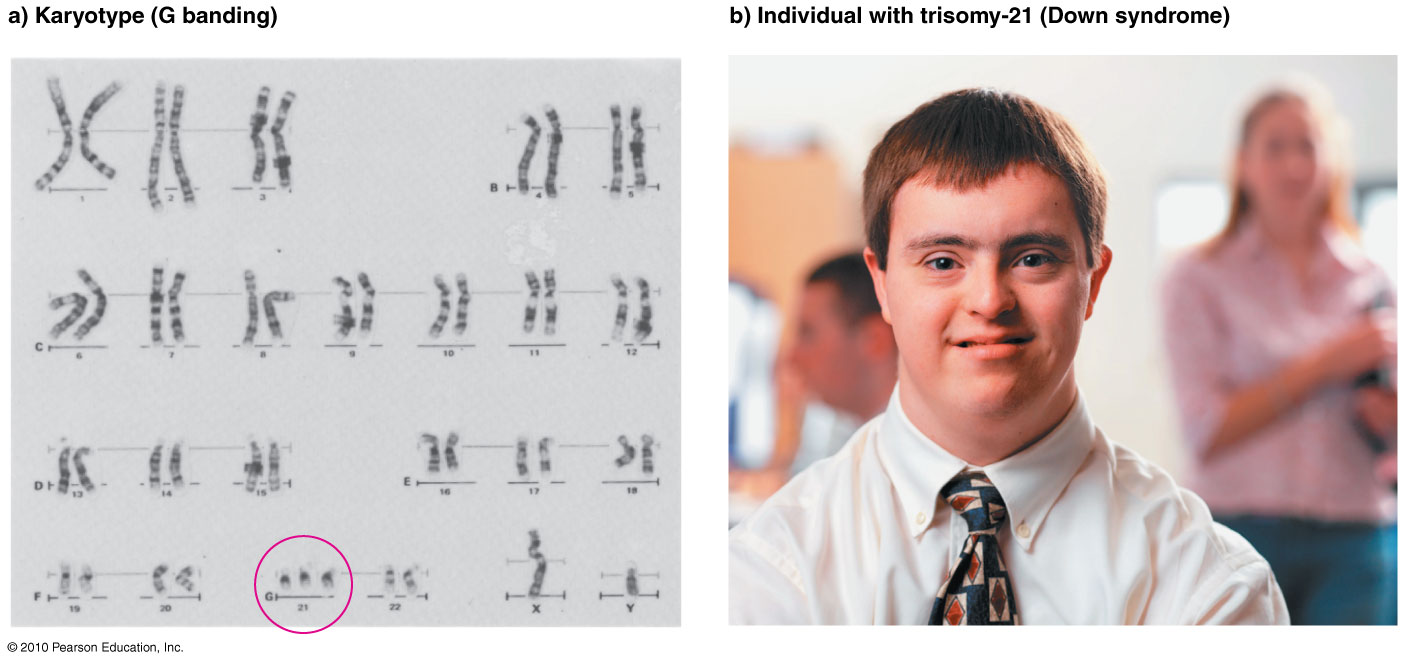
by one (unaffected) parent has two copies of Chromosome 21. When
fertilized by a gamete from the other parent, with a single
Chromosome 21, the result is a trisomy (three copies
of one chromosome: see G-banding karyotype). Trisomy
21 is the most common trisomy, and occurs in about 1 /
1,000 live births. The incidence is up to 50-fold higher in
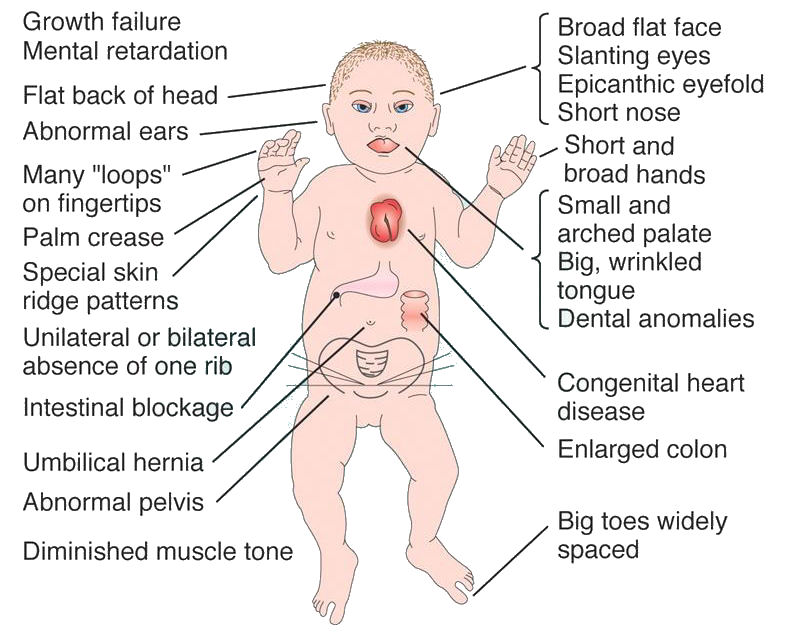
older mothers. The
syndrome is characterized by a distinctive facial phenotype
including epicanthic eye folds, a broad flat face,
characteristic palm crease, and moderate to severe
cognitive difficulties, as well as other medical conditions
noted above. The stereotypical
phenotype of persons with Down Syndrome is often
a white male with dark hair (see second photo), however Trisomy
21 occurs in both sexes and in all ethnicities. With
education and training, many persons with Down Syndrome
function well in the community. See the website of the Down Syndrome Research
Foundation [http://www.dsrf.org/home/]
for more information.
Most or all persons with Down Syndrome are functionally sterile, and do not pass on gametes with the duplicated chromosome to the next generation. Thus, although the condition is "genetic," it is not "inherited" in the same sense as are single-locus traits. Its random occurrence in the population is termed "sporadic". In very rare cases, Down Syndrome may result from a balanced translocation that attaches a substantial portion of Chromosome 21 to another chromosome (usually Chromosome 14) [this is indicated as 2n=46,t(q14q21)]. This form of Down Syndrome may be passed genetically (by asymptomatic, non-Down Syndrome parents) to the next generation. For this reason, it is advisable to check the karyotype of all persons with Down Syndrome, to provide appropriate genetic counseling.
Recent research suggests that the characteristic features of the Down Syndrome phenotype are due to the triplication of a small set of genes on Chromosome 21, rather than the trisomy per se. Selective re-regulation of the expression of one or a few key "Down Syndrome Critical Region"(DSCR) gene loci in utero might therefore provide an effective means of treatment. Study of the homologous genes in Drosophila may provide means to this end. A former US politician's trivialization of government-funded Drosophila research as irrelevant to human concerns is thus misinformed.
Prenatal diagnosis of Down Syndrome formerly used amniocentesis to recover fetal cells from the maternal amniotic fluid, which could then be cultured to check their karyotype. Testing was indicated with older mothers. Test results may not be possible until late in pregnancy. Several new DNA-based tests have been developed that use Next-Generation sequencing methods to diagnose Down Syndrome pregnancies much earlier in development.
Most or all persons with Down Syndrome are functionally sterile, and do not pass on gametes with the duplicated chromosome to the next generation. Thus, although the condition is "genetic," it is not "inherited" in the same sense as are single-locus traits. Its random occurrence in the population is termed "sporadic". In very rare cases, Down Syndrome may result from a balanced translocation that attaches a substantial portion of Chromosome 21 to another chromosome (usually Chromosome 14) [this is indicated as 2n=46,t(q14q21)]. This form of Down Syndrome may be passed genetically (by asymptomatic, non-Down Syndrome parents) to the next generation. For this reason, it is advisable to check the karyotype of all persons with Down Syndrome, to provide appropriate genetic counseling.
Recent research suggests that the characteristic features of the Down Syndrome phenotype are due to the triplication of a small set of genes on Chromosome 21, rather than the trisomy per se. Selective re-regulation of the expression of one or a few key "Down Syndrome Critical Region"(DSCR) gene loci in utero might therefore provide an effective means of treatment. Study of the homologous genes in Drosophila may provide means to this end. A former US politician's trivialization of government-funded Drosophila research as irrelevant to human concerns is thus misinformed.
Prenatal diagnosis of Down Syndrome formerly used amniocentesis to recover fetal cells from the maternal amniotic fluid, which could then be cultured to check their karyotype. Testing was indicated with older mothers. Test results may not be possible until late in pregnancy. Several new DNA-based tests have been developed that use Next-Generation sequencing methods to diagnose Down Syndrome pregnancies much earlier in development.




Carole, age 40; Children with Trisomy 21 competing at the Special Olympics; Catherine;
Abigail, from the exhibition "More Than Meets the Eye," St John's Arts & Culture Centre